 Your new post is loading...

|
Scooped by
rob halkes
|
Times are still good for the medical technology sector. Most companies still have strong gross margins, healthy growth in sales, and high valuation multiples. But the health care industry is undergoing a period of significant change. Medtech companies can take six actions to manage this transition and position themselves for long-term success. In the first few years of the 2000s—the golden age for medtech—sales grew by double digits. But sales growth has leveled off considerably in recent years and now hovers at around 4%. (See Exhibit 1.) There are many reasons for this, including the pressure to reduce health care costs, the increasing power of economic stakeholders in purchasing decisions, more consolidated and sophisticated health systems, new low-cost competitors, and the ubiquity of information with which to assess value. [...]
Times are still good for medtech—but the health care industry as a whole is undergoing a period of significant change. These changes could create a downward spiral for companies that cling tightly to business as usual. But those that build their capabilities and adapt their business models will find enormous opportunities to grow and thrive. In this report, we identify the major forces that are reshaping the industry and outline the transformative actions that medtech companies should take in response to them. We also describe how to manage such a transformational effort. By leveraging BCG’s proven transformation framework, medtech companies can improve their financial positions, close performance gaps, and establish a winning position.
|
|
Scooped by
rob halkes
|
A lot of people ask me about the future of medicine and healthcare. What’s coming next, what about the future of radiology, genomics or health sensors. They ask me to make really sharp predictions. But instead of this, let’s do something else now. Let’s look back from 2050, and see what today’s healthcare included, what barbaric elements played an important role in today’s healthcare in the 2010s.... See also here and here
|
|
Scooped by
rob halkes
|
PLAINSBORO, N.J. (PRWEB) July 16, 2015 -- The link between getting patients to take medication correctly and keeping down healthcare costs is strong enough that adherence is being tied to reimbursement for healthcare providers. A study published recently in The American Journal of Managed Care examines connections at the health plan level between good plan-level adherence, lower rates of disease complications, and lower medical spending.
|
|
Scooped by
rob halkes
|
|
|
Scooped by
rob halkes
|
Growth And Dispersion Of Accountable Care Organizations In 2015 | The Policy Journal of the Health Sphere David Muhlestein March 31, 2015 In January, an additional 89 provider organizations joined the Medicare Shared Savings Program (MSSP) as accountable care organizations (ACOs). While this year’s new entrants are a smaller cohort than those that joined in 2013 and 2014, they represent a continuation of the expansion of the accountable care movement. The recent Department of Health and Human Services (HHS) announcement of its goal to move 50 percent of Medicare payments to alternative payment models (including ACO-based arrangements) indicates the government’s strong backing of the model and, coupled with continuing endorsement of the approach from state Medicaid programs and commercial insurers, there is strong support for this care delivery approach to continue. In an ACO, health care providers accept responsibility for the cost and quality of care for a defined population. Each ACO’s laudable goal is to achieve what Don Berwick has called the “triple aim” — to improve quality, increase patient satisfaction, and lower costs. The key to reaching those goals is to change how providers are paid, based on reaching certain cost and quality benchmarks. In effect, the objective is to change incentives so that it is in providers’ best interest to maximize health, rather than focus on increasing the volume of services rendered. ACO GrowthLeavitt Partners has been actively tracking ACOs since 2010, maintaining a database that is updated regularly from publicly available information and personal and industry interviews. Over the past year, approximately 120 organizations have become ACOs in public and private programs, bringing the total to 744 since 2011 (Figure 1). The historical ACO growth data shown in Figure 1 are slightly different from our past estimates, as they are now based on the start date of the ACO’s contract, not on when the ACO was announced. For example, the 89 ACOs announced in December 2014 are listed as beginning in January 2015, which is the start of their contract. Regardless of how many contracts an ACO is engaged in, both public and private, an ACO is counted only once. Note that some of the new Medicare Shared Savings Program participants already had commercial contracts, and are thus tracked beginning at the start of their first contract. Figure 1. Total Public and Private Accountable Care Organizations, 2011 to January 2015 (See top)
Source: Leavitt Partners Center for Accountable Care Intelligence In addition to growth in the total number of ACOs, there has been continued growth in the number of people covered by ACO arrangements Read on the original blog here
|
|
Scooped by
rob halkes
|
This third edition of Health at a Glance: Europe presents a set of key indicators related to health status, determinants of health, health care resources and a
|
|
Scooped by
rob halkes
|
Approximately $6.5 billion in new funding flowed into the digital health space in 2014, more than double the previous year's haul of $2.9 billion, according to data from digital healthcare accelerator StartUp Health. But investors placed their bets on fewer companies. Only 459 companies received funding this year, a drop from the 590 who received investments in 2013. The decrease in companies financed is one of the “signs of a maturing market,” StartUp Health says. Another sign may be the stage at which venture capitalists and firms are making investments in startups. According to StartUp Health's data, just over 25% of deals were in the seed capital stage, a very early stage in a company's development. That's the lowest percentage since 2010, and indicates that there are relatively fewer funded startup entrants in this year's cohort.
Collectively, investors seem most enthused by big data and analytics, pouring $1.46 billion into 90 deals in 2014. Next was population health, with $1.14 billion invested.
|
|
Scooped by
rob halkes
|
This fact sheet describes the results of research into the factors influencing physician professional satisfaction and their implications for health care. The American Medical Association (AMA) asked RAND Health to identify the factors that influence physicians' professional satisfaction and describe their implications for the U.S. health care system. To do this, the researchers interviewed and surveyed physicians, allied health professionals, and other staff in 30 practices across six states, including a variety of practice sizes, specialties, and ownership models. Among the factors identified, two stood out as the most novel and important: - Physicians' perceptions about quality of care.Being able to deliver high-quality patient care was an overarching source of better physician professional satisfaction. Obstacles to providing high-quality care, such as lack of leadership support for quality improvement efforts, were major sources of dissatisfaction. These findings suggest that, in many cases, sources of physician professional dissatisfaction could represent important targets for quality improvement.
- Electronic health records (EHRs) Physicians noted that EHRs had the potential to improve some aspects of patient care and professional satisfaction. Yet for many physicians, the current state of EHR technology significantly worsened professional satisfaction in multiple ways, due to poor usability, time-consuming data entry, interference with face-to-face patient care, inefficient and less fulfilling work content, insufficient health information exchange, and degradation of clinical documentation. Some practices took steps — such as allowing multiple modes of data entry — to address a subset of these problems, but solving others (such as information exchange) may require industrywide cooperation.
|
|
Scooped by
rob halkes
|
World Health Organization Regional Office for Europe Health spending continues to outstrip the economic growth of most member countries of the Organisation for Economic Co-operation and Development (OECD). Pay for performance (P4P) has been identified as an innovative tool to improve the efficiency of health systems but evidence that it increases value for money, boosts quality or improves health outcomes is limited. Using a set of case studies from 12 OECD countries (including Estonia, France, Germany, Turkey and the United Kingdom), this book explores whether the potential power of P4P has been over-sold, or whether the disappointing results to date are more likely to be rooted in problems of design and implementation or inadequate monitoring and evaluation. Each case study analyses the design and implementation of decisions, including the role of stakeholders; critically assesses objectives versus results; and examines the “net” impacts, including positive spillover effects and unintended consequences.
With experiences from both high and middle-income countries, in primary and acute care settings, and both national and pilot programmes, these studies provide health finance policy-makers in diverse settings with a nuanced assessment of P4P programmes and their potential impact on the performance of health systems.
See the publication by McGrawHill here
|
|
Scooped by
rob halkes
|
A new settlement for health and social care - Final report This commission will ask whether the post-war settlement, which established separate systems for health and social care, remains fit for purpose. Download the final report from the Commission on the Future of Health and Social Care in England. Its 12 recommendations set out a vision for a more integrated health and social care service, simpler pathways through it and more equal treatment for equal needs. Key findings - The commission recommends moving to a single, ring-fenced budget for the NHS and social care, with a single commissioner for local services.
- A new care and support allowance, suggested by the commission, would offer choice and control to people with low to moderate needs while at the highest levels of need the battlelines between who pays for care – the NHS or the local authority – will be removed.
- Individuals and their carers would benefit from a much simpler path through the whole system of health and social care that is designed to reflect changing levels of need.
- The commission also recommends a focus on more equal support for equal need, which in the long term means making much more social care free at the point of use.
- The commission largely rejects new NHS charges and private insurance options in favour of public funding.
Policy implications - Proposals for a single, ring-fenced budget and single local commissioner will have major implications for central and local government and the NHS.
- Public spending on health and social care is likely to reach between 11 per cent and 12 per cent of GDP by 2025, the next government needs to consider how to respond to these spending pressures.
- The commission proposes funding changes, including changes to National Insurance contributions, to meet the additional £5 billion that would be required to improve social care entitlements.
- A comprehensive review of various forms of wealth taxation needs to be undertaken with a view to generating additional resources that will be needed for health and social care in future years.
Chris Ham blog "One of the great merits of the commission’s report is that it rises above the immediate pressures facing public finances to show that additional public funding is affordable." Read Chris's blog about the commission's final report See the summary on slideshare here
|
|
Scooped by
rob halkes
|
The tech giant's moves raise new questions about its plans to develop medical sensors. Emerging details about Apple’s forthcoming Healthbook app suggest the tech giant is asserting itself as a platform for digital health, a clearinghouse for data that could potentially prove as useful, revealing and lucrative as the ad profiles that drive the online economy today. The Cupertino company’s activities also raise questions about its plans to develop new medical sensors (possibly including a bloodless glucose monitor), integrate existing ones into forthcoming wearable devices or partner with companies developing these capabilities. “I wouldn’t be surprised if Apple has grand designs,” said Skip Snow, a senior health care analyst at Forrester Research. “They don’t usually do things on a small scale. But he and others said it was unclear whether Apple would come to dominate this space, as other tech companies are equally eager to plant themselves at the center of the health ecosystem — a sector that adds up to 17.9 percent of the nation’s gross domestic product.... It’s not certain how close to a final product Healthbook is or what it will look like when it hits the market. Early designs for the app appear to allow consumers to closely track health, fitness and activity information, as first reported by 9to5Mac and largely confirmed by Re/code’s own reporting. Apple declined to comment for this story... Why is Apple making such a big play here? Many observers believe we’re at the beginning of a transformation in health care, a consumerization of the space driven by the same online tools, apps and devices that have overhauled retail, media and finance. People have access to more information to make their own decisions about doctors, treatments and lifestyle choices... Of course, most of this is just potential for now. To date, companies developing wearables have seen significant attrition rates and have struggled to translate raw health data into genuinely useful information for consumers... “No average consumer knows what to do with the blood oxygen content from their finger,” Forrester analyst Frank Gillett said. “What they really want is something like, ‘Hey, you need you to take a walk today, and if you do that every day we’ll knock $5 off your insurance’ or something.” “So what we’re seeing,” he added, “are the foundation elements for something that may be more practical than the things we see in today’s activity-trackers.”
|
|
Scooped by
rob halkes
|
The following is a guest post by Atul Gawande, a surgeon at Brigham and Women’s Hospital, Professor at Harvard School of Public Health and Harvard Medical School, and Director of Ariadne Labs, in Boston. David Urbach and colleagues have recently published in the New England Journal of Medicine a study of what happened in Ontario after the government there mandated that hospitals adopt a surgical checklist that my research team at Harvard School of Public Health and the Brigham and Women’s Hospital had helped develop with the World Health Organization. This surgical checklist scripts that teams pause to discuss key issues before a patient is put to sleep, before the incision is made, and before the patient leaves the operating room—such as what the surgeon’s plan for the operation is, how long the case would take, how much blood loss the team should be prepared for, what medical issues the patient might have, and so on. In a trial in some eight thousand patients undergoing major surgical procedures in eight cities around the world, from Delhi to Toronto, complications fell by an average of 35% and deaths dropped 47%, as we reported in the New England Journal of Medicine (and I also reported in my book, The Checklist Manifesto).
Others have since verified the results both at small scale and at large scale. Neily et al. showed that a Veterans Administration program to implement the WHO Safe Surgery Checklist using a one-day team training method achieved a significant 18% reduction in mortality across 74 hospitals compared to controls. And in the Netherlands, after almost a year of implementation effort, the SURPASS trial showed that a comprehensive checklist approach achieved a 47% mortality reduction compared to controls. So what to make of the Ontario finding that three months after government-mandated adoption the drop in mortality rates failed to achieve significance? Well, I don’t honestly know. I wish the Ontario study were better. But it’s very hard to conclude anything from it. .. (read on) .. It has become clear that implementation takes time. In our original study, we tracked adoption, which proved far from perfect but at very small scale, in places with leadership eager to drive change, could be accomplished in weeks. ...(read on) .. My suspicion is that a government mandate without a serious effort to change the culture and practice of surgical teams results in limited change and weak, if any, reduction in mortality. But it’s hard to know from the Ontario study. Without measuring actual compliance with using the checklist, it’s like running a drug trial without knowing if the patients actually took the drug. Perhaps, however, this study will prompt greater attention to a fundamentally important question for health care reform broadly: how you implement an even simple change in systems that reduces errors and mortality – like a checklist. For there is one thing we know for sure: if you don’t use it, it doesn’t work.
|
|
Scooped by
rob halkes
|
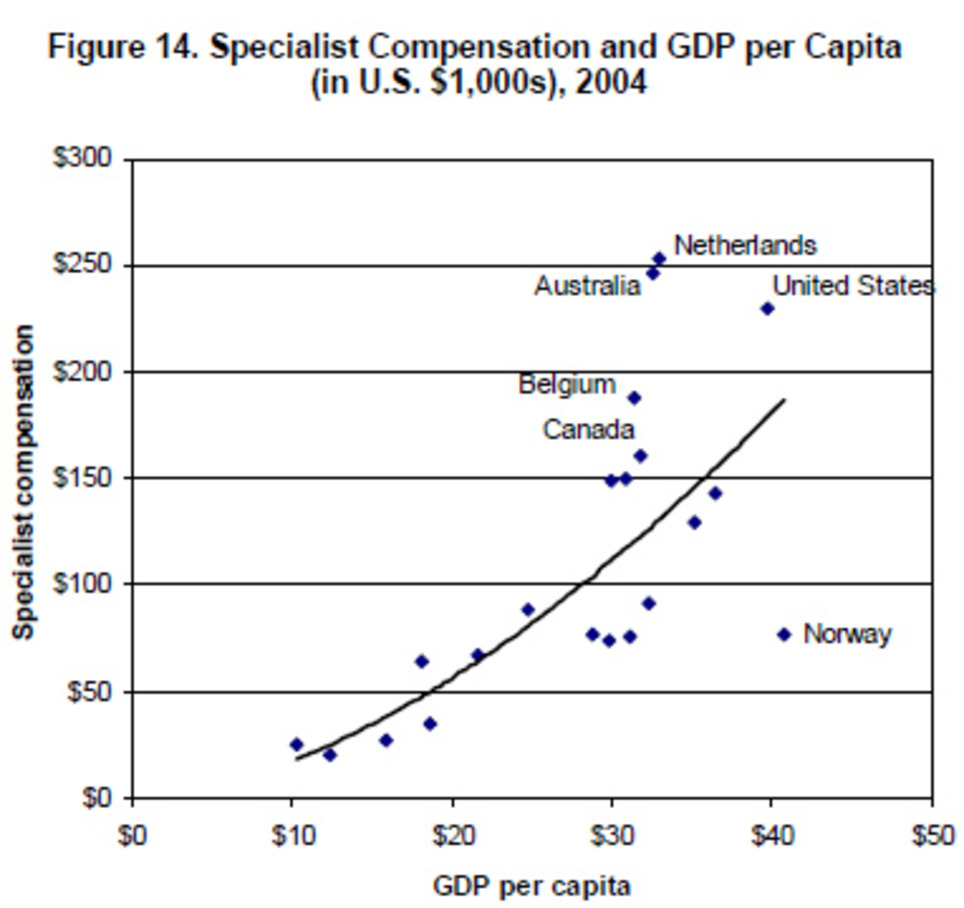
Two ways to compare physicians’ compensation in different countries. ... One way to compare cross-country data is to adjust the salaries for purchasing-power parity — that is, adjusting the numbers so that $1,000 of salary buys the same amount of goods and services in every country, providing a general sense of a physician’s standard of living in each nation. ... Another way is look at how a doctor’s salary compares to the average national income in that doctor’s country — that is, gross domestic product per capita. ... As a country’s wealth rises, so should doctors’ pay. But even accounting for this trend, the United States pays doctors more than its wealth would predict: (See graph) According to this model, the 2007 report says, “The U.S. position above the trendline indicates that specialists are paid approximately $50,000 more than would be predicted by the high U.S. GDP. General practitioners are paid roughly $30,000 more than the U.S. GDP would predict, and nurses are paid $8,000 more.” But it’s important to keep in mind, the report notes, that health care professionals in other O.E.C.D. countries pay much less (if anything) for their medical educations than do their American counterparts. In other words, doctors and nurses in the rest of the industrialized world start their medical careers with much less student loan debt compared to medical graduates in the United States. For more data on health spending in O.E.C.D. countries, go here. For a recent American-only survey on the pay of physicians with various specialties, go here.
|
|
Scooped by
rob halkes
|
Dr. Pierre Theodore of UC San Francisco has completed a three-month trial using Google Glass during surgery. For a little over three months now, Dr. Pierre Theodore, a cardiothoracic surgeon, has been using Google Glass in the operating room. Although he's tapped the functionality during procedures on just 10 patients, for various cancer mass removals, fluid removal, and a lung restoration, Theodore (who we first wrote about in August) may have more experience using Glass in a serious medical setting than any other doctor in the world. His conclusion so far: the technology is indeed useful in the operating room as an adjunct device in delivering necessary information, but it still has miles to go as a product.... Read on!
|
|
Scooped by
rob halkes
|
The personal health budget (PHB) is the most revolutionary expression of personalisation ever introduced to the NHS. It embodies and epitomises the Government’s vision of a patient-centred NHS, summed up by the often quoted edict ‘no decision about me, without me’. Yet it is impossible to ignore professional concern and disquiet around the implementation of PHBs. This report responds to some key fears and objections with learning and best practice emerging from the pilot programme. This report was funded by an unrestricted educational grant from Denplan. We are indebted to Denplan who enabled this research to be undertaken, and to all our sponsors. As well as driving our on-going work of involving frontline professionals and the public in policy ideas and development, sponsorship enables us to communicate with and involve officials and policymakers in the work that we do. Involvement in the work of 2020health is never conditional on being a sponsor. Also download reference to the report. DO!
|
|
Scooped by
rob halkes
|
This PwC Health Research Institute (HRI) report looks at the projected increase in the cost of medical services for 2014. Read how medical cost trends affect your business. For 2014, PwC's Health Research Institute (HRI) projects a medical cost trend of 6.5%. Defying historical patterns—and placing added tension on the health industry—medical inflation in 2014 will dip even lower than in 2013. Aggressive and creative steps by employers, new venues and models for delivering care, and elements of the Affordable Care Act (ACA) are expected to exert continued downward pressure on the health sector .. Healthcare organizations, hurt by a squeeze on reimbursements and what might best be described as a recession “hangover,” have spent the past few years adapting to more modest growth rates. The industry will continue those efforts in 2014, including pushing care to locations and personnel that cost less...
|
|
Scooped by
rob halkes
|
There's scant evidence that these programs improve outcomes. While health spending in the United States far surpasses that in other industrialized nations, the quality of care in the US is no better overall, and on several measures it is worse. This stark fact has led to a wave of payment reforms that shift from rewarding volume (as fee for service does) to rewarding quality and efficiency. Such pay-for-performance schemes seem to be common sense and are now widely used by private payers and Medicare. But astonishingly, there’s little evidence that they actually improve quality. What do we really know about the effectiveness of using financial incentives to improve quality and reduce costs in health care? There is robust evidence that health care providers respond to certain financial incentives: medical students have a higher demand for residencies in more lucrative specialties, physicians are more likely to order tests when they own the equipment, and hospitals seek to expand care for profitable services at the expense of unprofitable services. It would seem that increasing payment for high-quality care (and, conversely, lowering payment for low-quality care) is an obvious way to improve value in health care. But evidence suggests that health care is no different from other settings where similar payment incentives have been tried, such as education and private industry. Not only do these payment policies often fail to motivate the desired behaviors, they may also encourage cheating or other unintended responses. Overall, evidence of the effectiveness of pay-for-performance in improving health care quality is mixed, without conclusive proof that these programs either succeed or fail. Some evaluations of pay-for-performance programs have found that they can modestly improve adherence to evidence-based practice. There is little evidence, however, that these programs improve patient outcomes, suggesting that to the extent that health care providers have responded to pay-for-performance programs, that response has been narrowly focused on improving the measures for which they are rewarded — such as making sure patients receive recommended blood tests if they have diabetes or the right cocktail of medications if they are hospitalized with a heart attack. Although these measures are important for patient care, it may take a full reengineering of the health care delivery system to broadly improve patient outcomes. ..read on..!
|


























Times are still good for business in med tech.. for pharma and healthcare provision as well. But the large BUT is indeed health care as a whole is undergoing significant changes. When these (market) and system changes are not paralleled by internal changes in the health industry companies, I guess it will get tricky before 2020. See here how you can cope